I pulled a George R.R. Martin: I promised a quick follow-up to Part 1 of this series written six months ago, and just now forced myself to finish it. I'll blame some of that lovingly on my son, who was born in mid-2022 and took up nearly every ounce of my spare time since (worth it). But I also struggled with how to write about this particular topic. Explaining how healthcare organizations are paid in a succinct and engaging way is HARD, and I bored myself to death with several false starts on it. Fortunately, I finally found a way to merge my favorite city and one of my favorite video games into an apt comparison of how I view the subject.
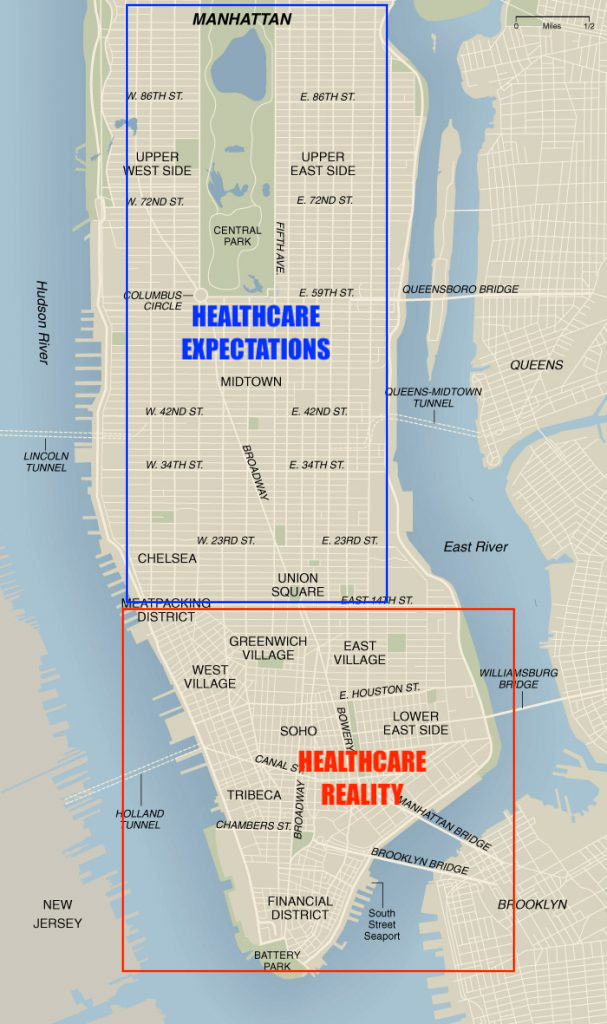
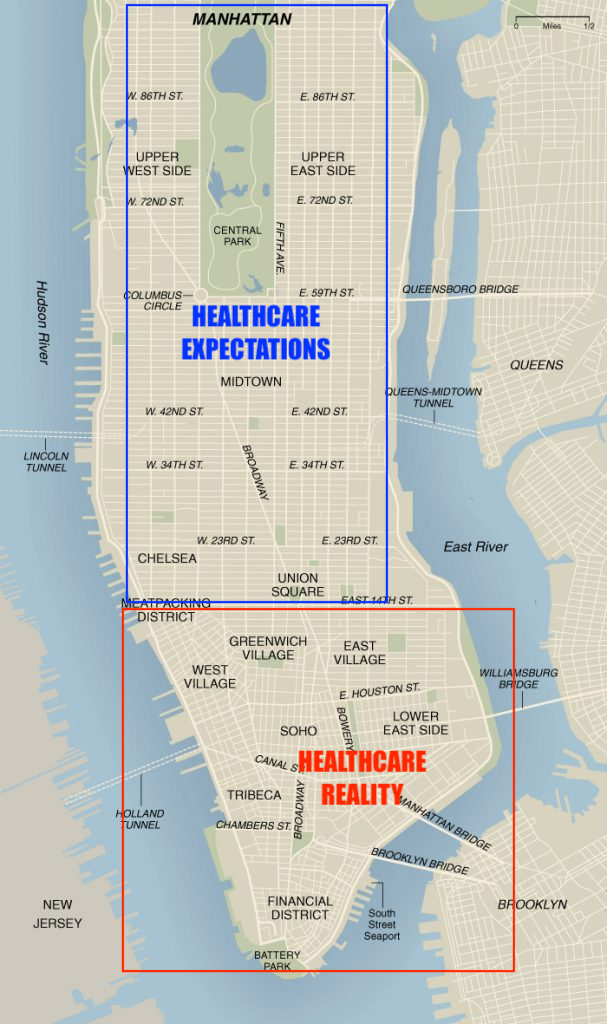
The 14th Street Divide
If you work in healthcare and have either lived in NYC or frequently travel there, then you probably know where I'm going with this. The Manhattan street grid system is a wondrous marvel: a rectangular mosaic of avenues (North / South) and streets (East / West) that, once you acclimate to the high-rise vertigo, is simple and intuitive to navigate. Feeling lost in midtown on your way to Central Park? Just find 5th - 8th Avenue and walk "New York North" (technically north-northeast on an actual map) and you'll hit that magnificent green-space. Want to enjoy the breeze of the Hudson River with a New Jersey background? Just walk westward and keep an eye on the Avenue increase – once you hit 10th, you're getting close. It's such a simple and practical design across all of Uptown and Midtown: up, up, down, down, left, right, left, right (B, A, Start). Easy peasy... until you get to Downtown.
On the lower border of Midtown lies 14th Street, the last bastion of perpendicular logic in the city. Below that is Downtown, and when you step foot into it, the once rectangular grid starts to look like The Mirror Dimension. Numbered street and avenue names give way to vague names alluding to random people and places, likely accounting for property lines belonging to wealthy New Yorkers of old. By the time you get to Lower Manhattan, the streets run at all angles, and it's easy to get lost within a one-mile radius. It makes no damn sense.
So why am I talking about navigating a concrete jungle while this post is supposed to be about healthcare? Because I need to drive home the analogy, especially for unfamiliar readers, about just how ridiculously complex the industry is when it comes to how healthcare facilities (aka, organizations) are paid. I stress the word facilities because being paid as a practitioner is relatively straightforward in comparison. Practitioners – an individual human with a National Provider Identifier (NPI) – can bill on their own (NPI Type 1), but it's far more common to have the facilities they are affiliated with submit a bill (NPI Type 2). Facilities can be group practices with multiple doctors, hospitals, multi-specialty clinics, radiology centers, and nursing homes – the list is quite long.
Every type of healthcare facility has a different rule-set on what can be billed, how the bill should be submitted, and how much is reimbursed. Each year the rules can change, and they often do.
But Jason, it can't be that bad... can it? It shouldn't be, but it is. To drive the point home, I present the only evidence you'll need: The Medicare Claims Processing Manual. This 39-chapter manual is so large that CMS has divided each chapter into a separate PDF. The Inpatient Hospital Billing chapter is 387 pages long; Durable Medical Equipment is 115 pages; "How to File and Appeal" is 103 pages; you get the point, and the entire manual is over 1,000 pages. The chapter on practitioner payments, while also long at 192 pages, is relatively self-contained, and might be all you need to read if you want to run a single-member LLC practice in a rural town. But alas, that's not the path taken by most practitioners.
No amount of finesse can make this type of content fun to read, but if you're a glutton for punishment, then I suggest you browse that manual and count the days until your hair starts to turn grey. But remember, we're still talking only about Medicare. Things get even worse from here, and payment calculations in the Commercial world quickly get more confusing than the plot of TENET.
Bloaters and Rat Kings
Given the popularity of The Last of Us on HBO as I write this, I'll give you a comparison on Medicare vs Commercial claims payment complexity. Medicare payments are much like that huge bloater from Episode 5 that climbs out of the ground: he's old and practically indestructible, is a necessary evolution of his younger clicker counterparts, and non-players of the game will think: this must be as bad as it gets with the infected, right?
Unfortunately, I have bad news for you: the mutation gets even worse. Most commercial plans use the Medicare payment manual as a baseline, then order their actuaries to come up with even more convoluted benefit structures that become nearly impossible to interpret from those on the outside. Then, those same plans often have to navigate through difficult pricing negotiations with providers, many of whom are being run by private equity firms trying to squeeze every last drop of margin from their portfolio companies, often to the detriment of patients. This winner take all mentality results in new ideas awkwardly fused onto old ones, resulting in a malformed monstrosity. In other words, the (SPOILER ALERT) Rat King from The Last of Us 2. What an ugly bastard.
Here's a few real-world examples of just how convoluted things can get:
In some primary care clinics with multiple physicians, some physicians may be in-network for a given health plan while others aren't.
A provider might be in a health plan's network for one plan type in a market, but not for another. For example, local hospital might be in-network for Cigna's employer sponsored insurance plans, but not for Cigna's individual plans sold on the federal exchange in the same market.
A fee schedule (aka, a list of procedures and reimbursement rates) might have something like "150%" of Medicare for a procedure category (ie, Imaging, Surgery), but there might carve-outs where specific codes are paid at 200% of Medicare.
An in-network hospital might use a physician staffing firm where the ER practitioners, while working at an in-network hospital, are out-of-network at the practitioner level. This means you could get hit with an Anesthesia bill that costs more than your actual hospital visit. (This has been somewhat mitigated via the No Surprises Act, but the example is worth noting.)
A facility might be out-of-network for a given health plan, but that facility might have negotiated a direct contract with a given employer that makes it in-network, and the contract is between the facility and the employer instead of the health plan and the employer.
None of these examples even touch on other negotiation tactics such as capitation, bundled pricing, reference-based pricing, and value-based care (paid via health outcomes). Each of these adds another permutation to the payment layer, creating job security for people like me that have spent a decade learning how all this shit works while leaving patients confused and frustrated at their own health plans.
Monsters in FiDi
I hope by now that you're visualizing bloaters and rat kings wondering aimlessly down the streets of Lower Manhattan's Financial District. Other than making for an excellent plot in The Last of Us Part 3, this mash-up perfectly represents – to me, at least – the complexity and bloat of a system that evolved from practical beginnings to it's current ostentatious display. Acknowledging this is important, because it sets the stage for why the machine-readable files mandated by CMS haven't been the immediate panacea to our healthcare pricing woes that so many people were hoping for. There's definitely a sliver of light now at the end of the tunnel, but that light is still small and dim, and getting through to the other side is going to take a lot more work than people realize. More on that in the next post as we conclude this series.