It's hard to communicate how much AI has impacted pharmacology- especially inside Europe’s famously cautious, highly regulated environment. The AGAH conference, the intimate heartbeat of the German-speaking clinical pharmacology community, chose the perfect title this year:
“Optimism, Courage, and Pragmatism – Human Pharmacology 2030”. The message was unmistakable: the future isn’t coming .... it’s already here, and we’d better drive it.
The program was a manifesto:
- Model-Informed Drug Development – Progress and Outlook - Dose Selection for Phase 2 and Phase 3 – Optimal and Optimus - Overly Complex Early Phase Trials – Proposals for Improvement - Artificial Intelligence Impacting Clinical Pharmacology – A Dynamic Field of Opportunities - Regulatory Enablers of Innovative Early Medicines Development
What struck me most was the mindset shift. Senior voices from big pharma were no longer staying in their lanes. They were talking about “the big story of the drug.” and connecting this to critical thinking where the Human is better than AI. This has been the first time I have heard pharma openly reflect on "we want to use more MIDD" to "Let's get responsible and understand what we are aiming for". For the first time I saw the shift in needing to be useful.
Day 1: MIDD in Action — ICH M15, Real Regulatory Wins, and the Politics of Modelling Tools
ICH M15 (the new guideline on context-of-use for models) was talked about and gently stress-tested. Everyone welcomed the framework, yet speakers noted that as drugs become more complex (bispecifics, cell therapies, rare diseases), the “context-of-use” bar will be tough to maneuver.
Stand-out regulatory success stories:
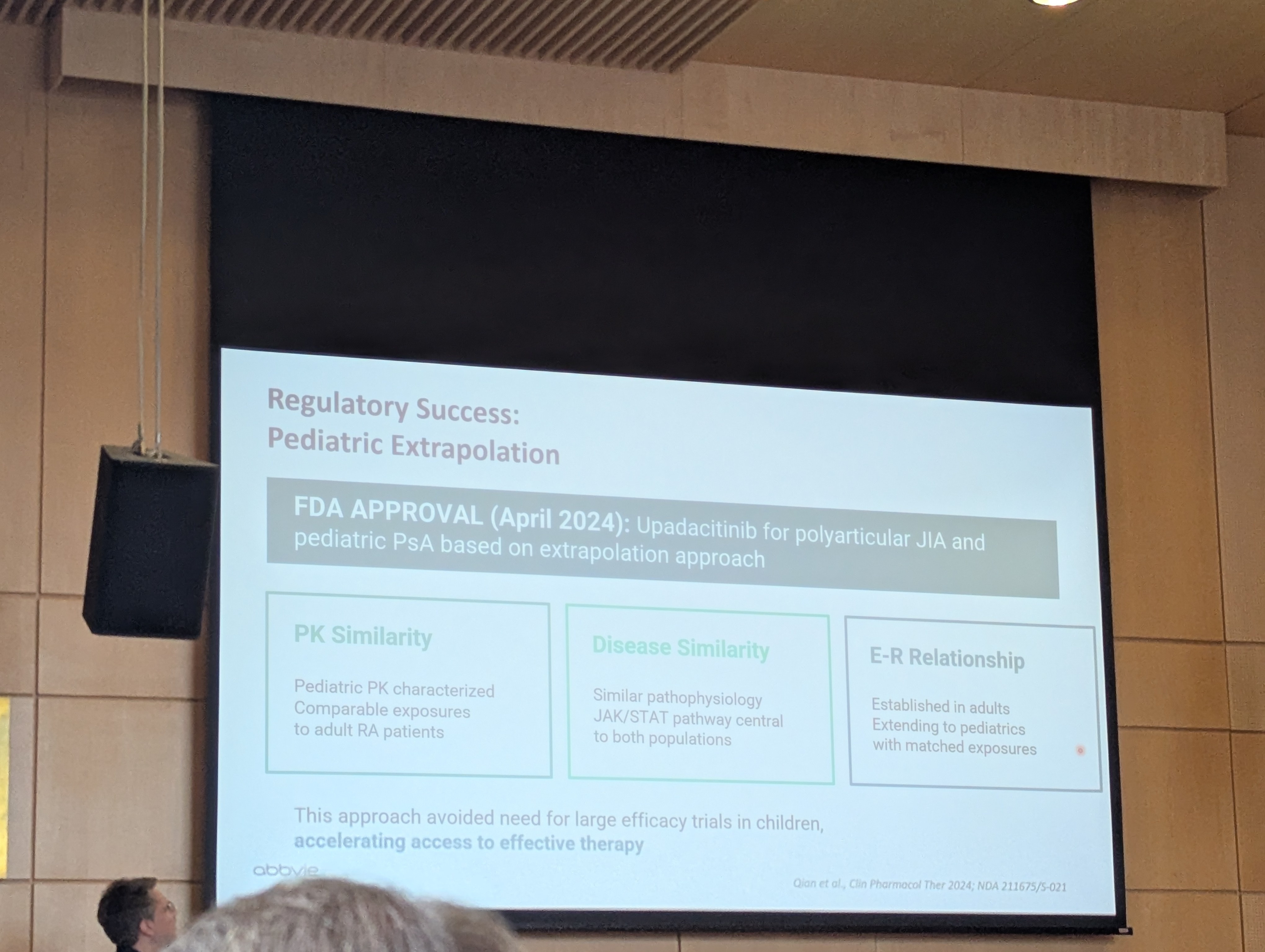
- AbbVie presented the upadacitinib pediatric extrapolation that secured FDA approval in April 2024 for polyarticular juvenile idiopathic arthritis (pcJIA) and pediatric PsA. Their slide laid a really cool and clear case of: PK Similarity + Disease Similarity + E-R Relationship using time-continuous Markov chain models on adult RA data. No large new pediatric efficacy trials needed. This was a mix drop moment- a classic case for which MIDD is built for.
- Merck gave the strategic overview: open to any approach (empirical, mechanistic PBPK/QSP, AI hybrids) as long as context-of-use is rock-solid.
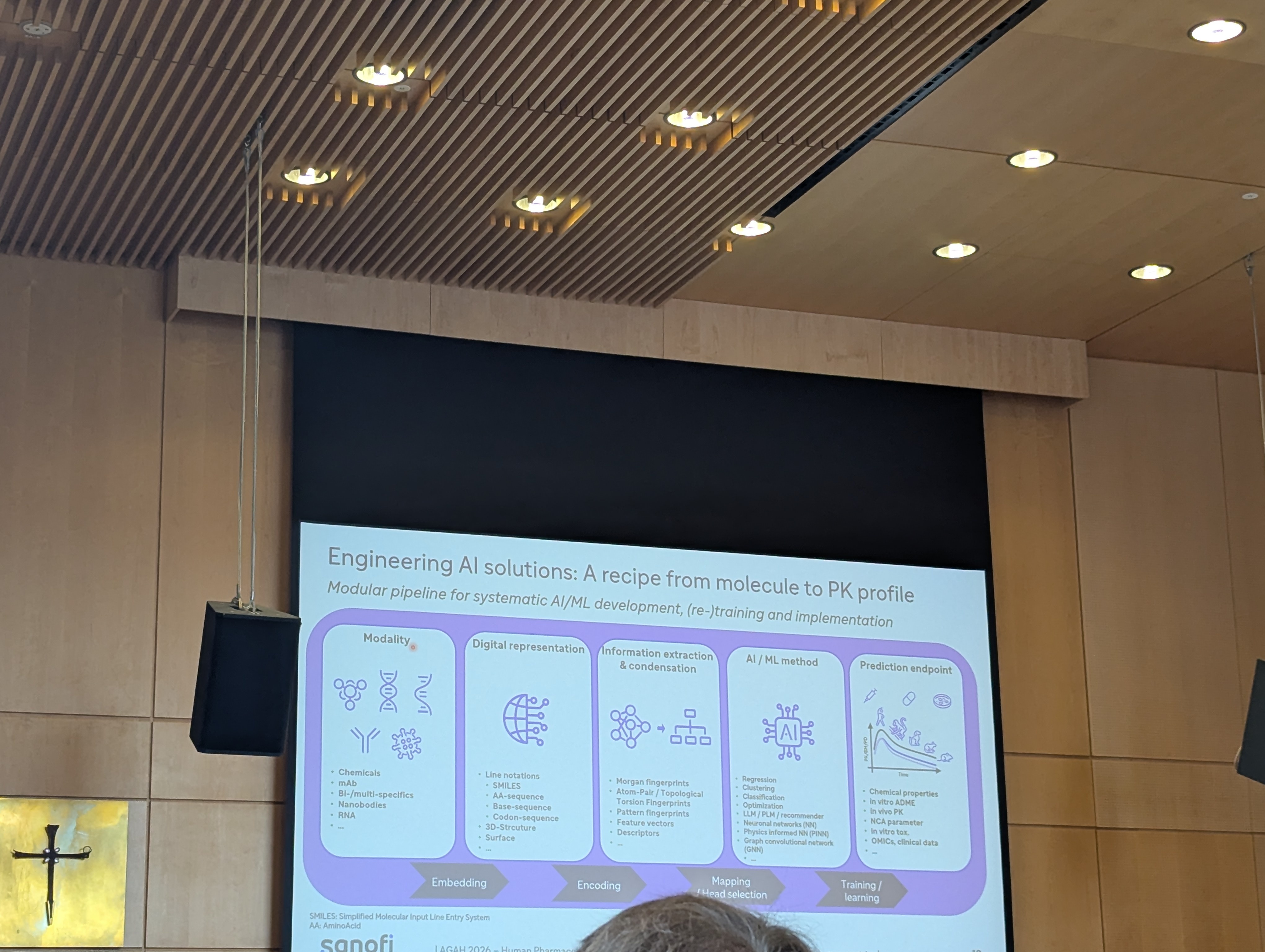
- Sanofi showed how they’re finally wiring AI into the full DMTA cycle. It was pleasant to see they are also finally integrating their modelling workflows toge her more tightly. The modular pipeline slide — from molecule modality → digital representation → AI method → prediction endpoint — felt good to see that there is more of tangiable follow on MIDD in early discovery.
A fascinating undercurrent: in the MIDD space, small modelling vendors have passionate champions. Open-source tools were proudly named. Competing commercial platforms were either omitted or quietly footnoted. I think AI will change that drastically. Democratization of tools is going to be the flag of AI and of course that would also mean people will have to move from "one loyal camp" to "many loyal camps" and root for some of the most useful products.
A full session was dedicated to dose-finding projects, with two talks focused squarely on Project Optimus (FDA’s initiative to move oncology development away from the traditional maximum tolerated dose [MTD] paradigm). One of the leading pharmacometrics academics- Bernd Meibohm (University of Tennessee Health Science Center) delivered a standout academic perspective in his talk on “The Value Continuum of PKPD: From Post-Marketing to Preclinical Development”. He emphasized that dose optimization must be viewed as a lifecycle continuum, not a single Phase 1 decision.
The ethics-committee and protocol panel was brutally honest. Germany, France and Spain dominate early-phase sites; Spain’s surge is cost-driven. The consensus? “We optimise for inspection and ethics, but we’ve added too much noise.” Simplify. Remove what doesn’t add signal.
Day 2: AI Front and Centre — Bayesian Learning, QbD, QSP, and Regulatory Enablement
This was the day for me particularly when the room lit up.
BfArM showed a slide titled “Bayesian Inference for Randomization” that perfectly captured the paradigm shift:
> In a traditional trial, randomization is fixed (e.g., 50/50). In a Bayesian Adaptive Trial, the system *learns* as it goes.
Bullets: ► Prior Knowledge → initial belief ► New Data → patients join, results come in ► Inference → probability that Treatment A is better ► Adaptive Randomization→ automatically shifts future patients toward the winning arm.
Simple. Powerful. Game-changing.
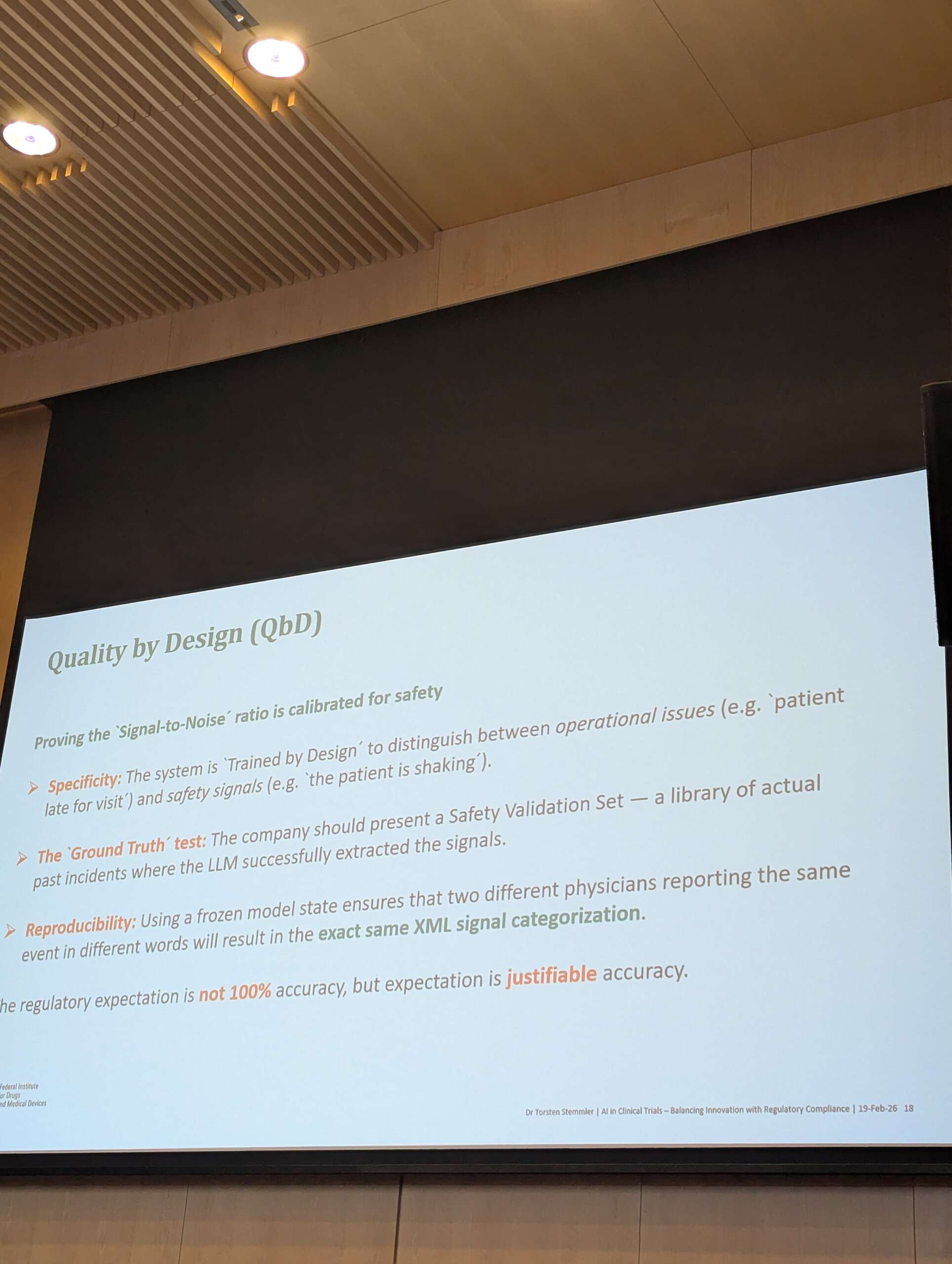
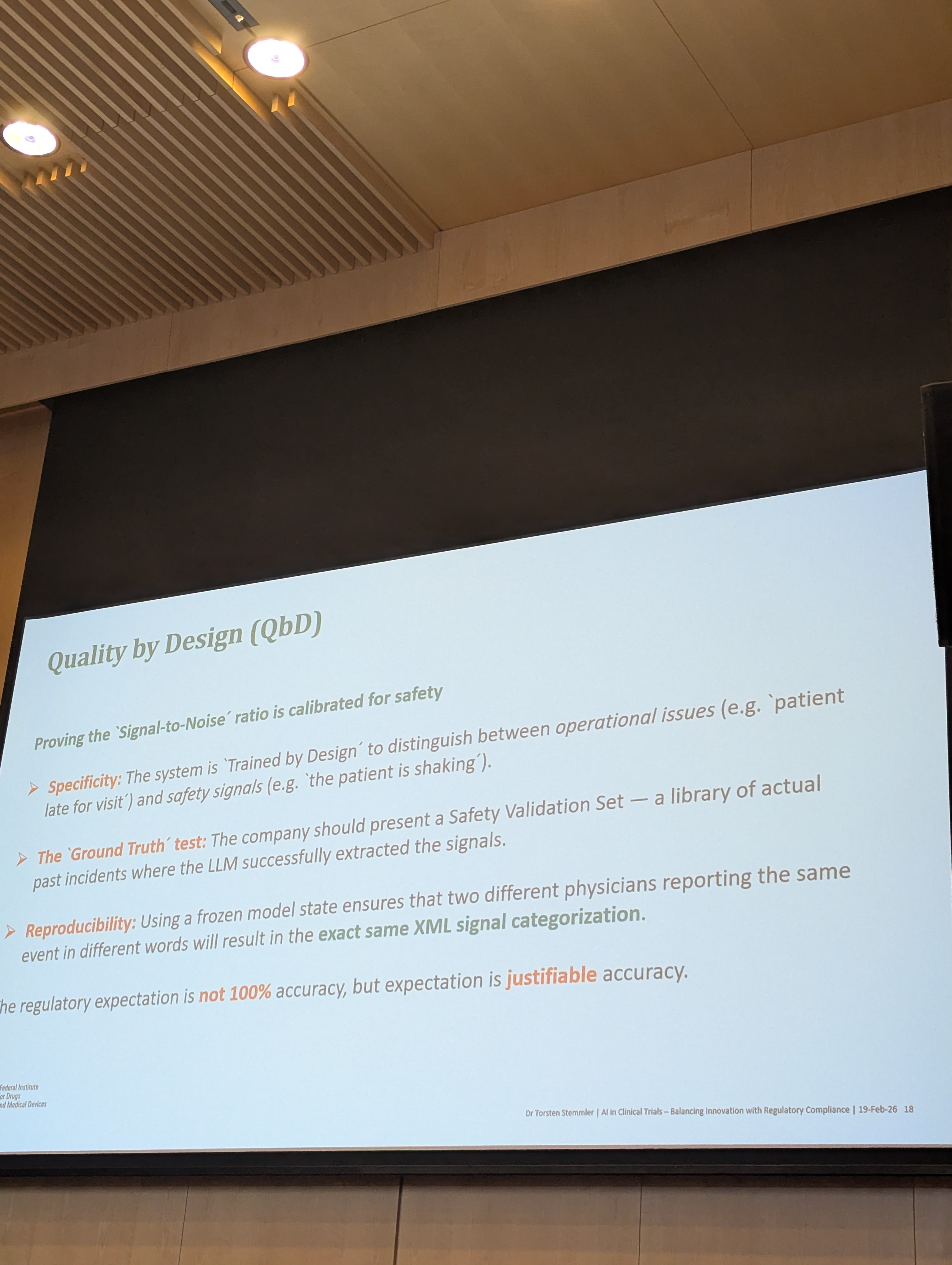
Right after, another BfArM slide on Quality by Design (QbD) for LLM-based safety-signal extraction: “Proving the ‘Signal-to-Noise’ ratio is calibrated for safety.” Specificity, ground-truth validation set from past incidents, frozen model for reproducibility, and the killer line in orange: “The regulatory expectation is not 100% accuracy, but expectation is justifiable accuracy.” Regulators and sponsors nodded in unison.
Nova Insilico positioned "QSP as a middle ground” — biology-grounded, white-box, parsimonious, versatile across in-vitro/animal/clinical/real-world data, and modular with AI accelerators for literature extraction and code writing. The accompanying diagram of an acute myeloid leukemia QSP model (stem cells → progenitors → blasts, with patient-specific and clone-specific parameters) was an example of successful data extraction and building equations.. at least semi autonomously where AI can support as a tool. There were many critical thinkers who also had the opinion to not trust AI like for example the belief of not wanting to make it write for you because it makes you become complacent. The Bfarm was also very clear on human complacency in this regard as they spoke about acceptance bias which is high in humans (where for example if they have to click allow more than 10 times they will make a mistake by continuing to do so out of habit).
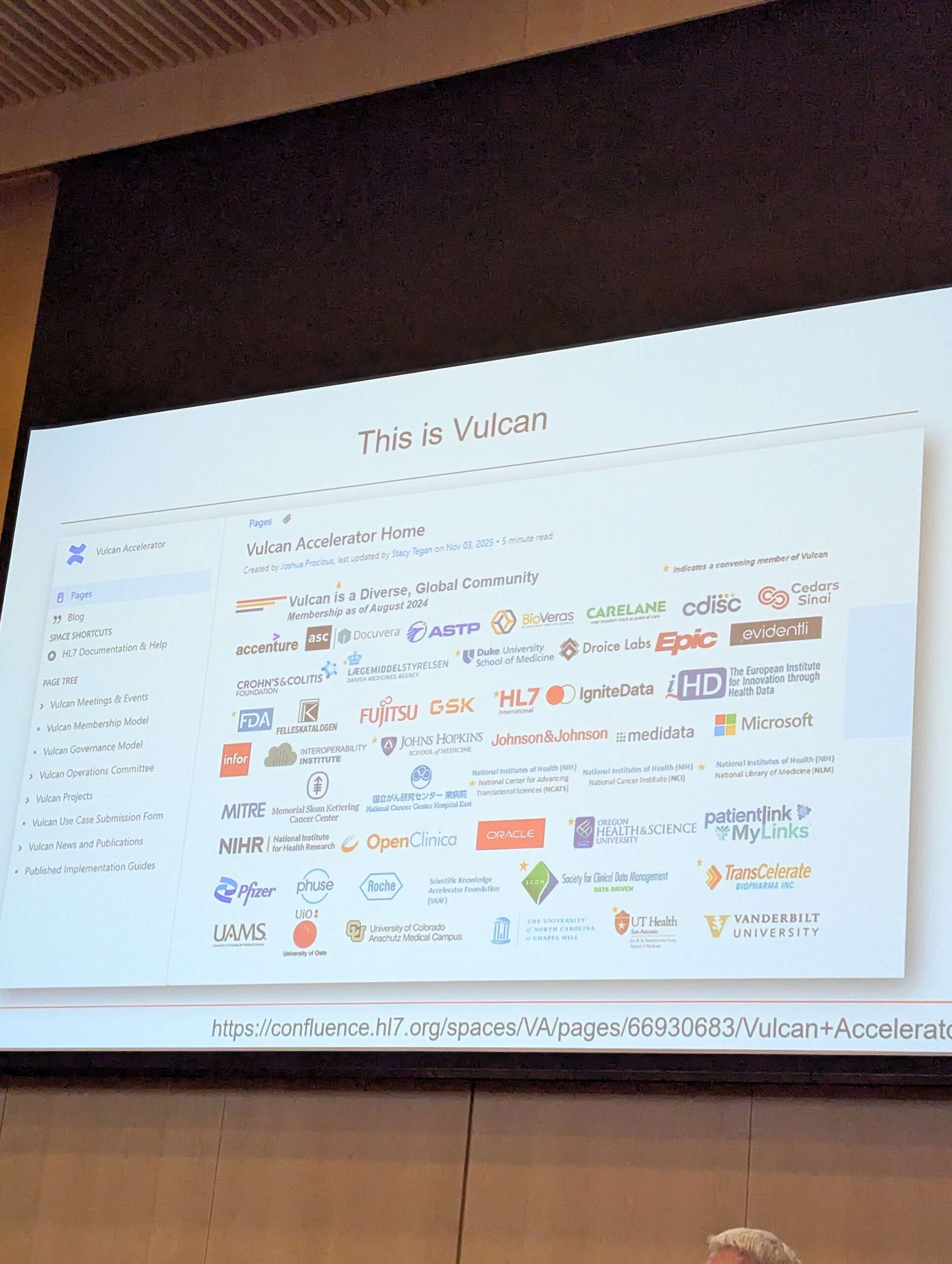
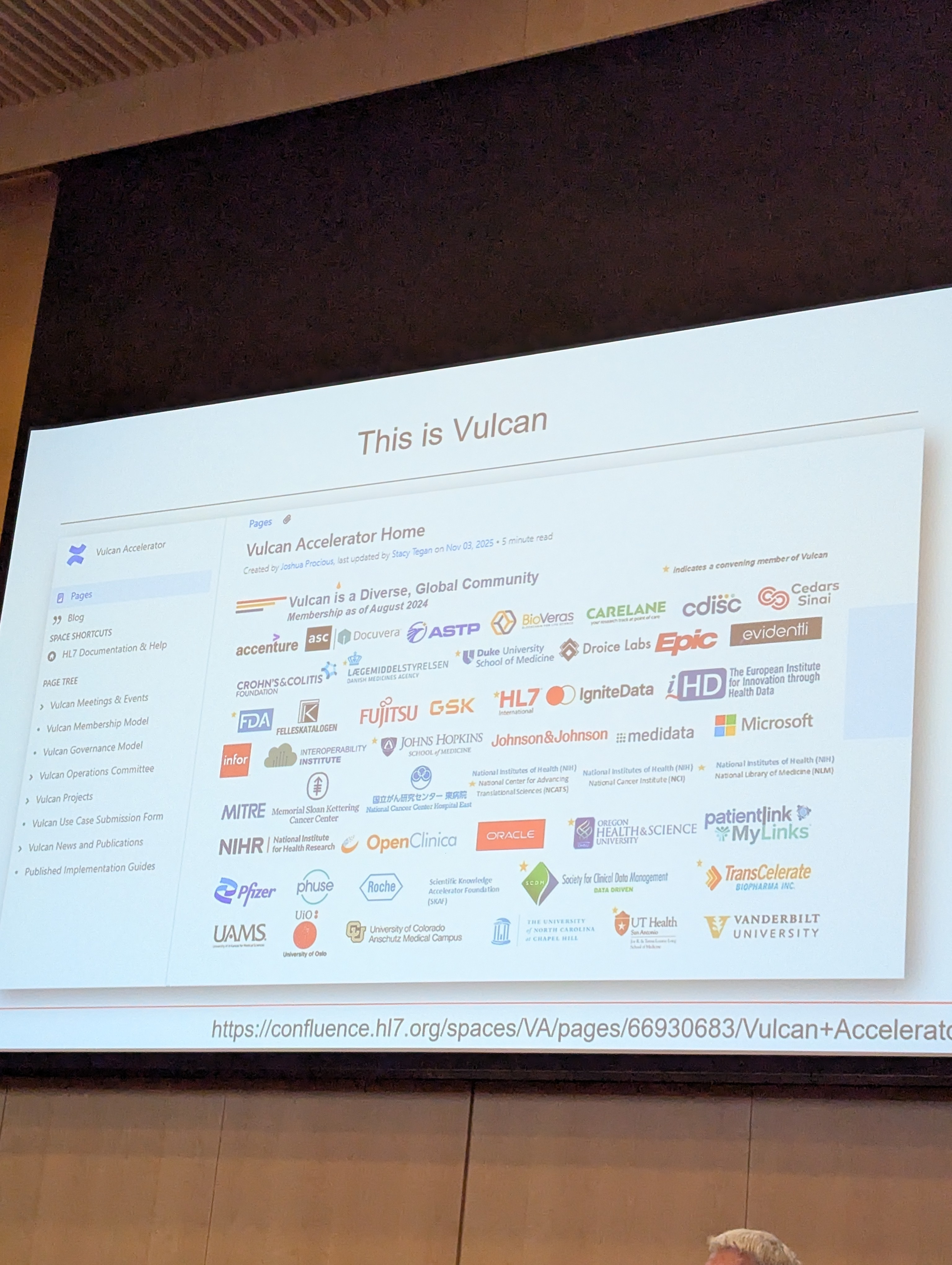
Bayer talked about AI in stdy protocols and here Vulcan, the HL7/FHIR/CDISC/ICH M11 initiative for digital protocols, got its own spotlight. One slide showed the massive participant list (FDA, Pfizer, Roche, Microsoft, Johns Hopkins, etc.). Another highlighted the project title in red: “Vulcan FHIR® Accelerator Connects CDISC, HL7, and ICH M11 in a Project to Digitize Exchange of Clinical Research Protocols" — creating the Clinical electronic Structured Harmonised Protocol (CeSHarP). The vision: fully machine-readable protocols flowing straight into submissions.
The Real Story: A Cultural Mindset Shift
The deepest impression wasn’t any single algorithm. It was the culture change.
Big pharma is building interconnected ecosystems: literature → QSP → PBPK → trial simulations → dose selection → regulatory strategy. People are explicitly connecting critical thinking to “the big story of the drug.”
For the first time, the most conservative pharmacologists are zooming out because AI has knocked so loudly on the door.
BfArM on GenAI sponsor use, Sanofi’s PINN success, Nova’s prospective FLAURA2 prediction, AbbVie’s pediatric approval without new trials ... all pointed the same way. One slide even quantified it: MIDD approaches yield average savings of several months cycle time and $5 million per program.
And the German-speaking clinical pharmacology community — traditionally so measured — just gave it a warm, pragmatic, and quietly optimistic welcome.
I wonder- a lot. So, I write my wonder here. What to expect? The chaos and curiosity that my being brings. As living a human life is not bound by definitions in the macros- the posts here will be spontaneous and identity-less! I like to give and create art. So if you buy an act of creating I will use it for things that I am passionate to give for. Obviously, a little support on my art will make me feel visible.
"Change. Change. Change. Change … change. Change. Chaaange. When you say words a lot they don't mean anything. Or maybe they don't mean anything anyway, and we just think they do."