Attending the 34th PAGE (Population Approach Group Europe) Meeting in Dubrovnik, Croatia, in June 2026 was an int resting experience for me. It was my first time at this prestigious gathering, and I arrived with high expectations shaped by years of following the field from afar.
What I encountered surpassed them: a community not only deeply engaged in rigorous quantitative science but also actively steering pharmacometrics toward greater mechanistic depth, computationally aware and really strong on communal belongingness.
The stunning Adriatic backdrop provided a fitting stage for discussions that revealed a field in clear transition: from describing clinical data with relatively simple compartmental models to building explanatory, physiologically grounded frameworks that integrate decades of accumulated biological knowledge.
There is a silent shift in pharmacometrics from empirical description to mechanistic explanation, not toward pure machine learning or hybrid ODEs. This directly challenges the investment thesis that insilico AI will render deterministic PK/PD obsolete.
Mechanistic modeling dominated the scientific program. Pregnancy PBPK-PD frameworks for monoclonal antibodies integrated FcRn-mediated IgG recycling, placental transfer dynamics, and gestational physiology across trimesters, incorporating allometric scaling and in vitro binding data.
QSP platforms for metabolic disease linked multi-organ systems: CNS regulation, hepatic GLUT/insulin signaling, adipose energy balance, and gut hormone feedback: through differential equations.
There were parallel open source efforts that reconstructed advanced dissolution-absorption-metabolism (ADAM) models in open platforms like R, with explicit segmentation of the gastrointestinal tract, mechanistic handling of dissolution, precipitation, efflux, and metabolism. These were benchmarked against established tools such as Simcyp and PK-Sim, highlighting how structural assumptions influence predicted kinetics and underscoring the value of transparent, customizable implementations. And all things arise in the gut. Coming to open source there is a Rust based implementation for PKPD modelling and the cool part is that they have lots of different kinds of estimation and sampling method.
This evolution is not merely technological; it reflects the natural maturation of a discipline. In earlier eras, when clinical datasets were sparse and biomarkers limited, empirical or semi-mechanistic PK/PD models served as essential tools for characterizing exposure-response relationships. Today, with richer physiological understanding, multi-omics insights, and advanced computational power, researchers are constructing models that explain why phenomena occur.
The posters and presentations at PAGE 2026 made this shift extremely visible. Multiple groups presented sophisticated PBPK-PD models for pregnancy, capturing FcRn-mediated IgG recycling, placental transfer dynamics, and maternal-fetal concentration gradients for monoclonal antibodies such as Rozanolixizumab and Nipocalimab. These models integrated in vitro binding data, allometric scaling from cynomolgus monkey studies, and physiological changes across gestation weeks 14–35, with validation against both healthy volunteer and patient data, including compassionate-use cases. The result is not just better prediction but genuine mechanistic insight into how drug disposition changes in one of the most vulnerable populations.
The same spirit of mechanistic ambition appeared in Quantitative Systems Pharmacology (QSP) models of metabolism. Detailed multi-organ frameworks incorporated CNS neuron regulation, adipose energy balance, liver GLUT/insulin dynamics, muscle protein turnover, gut hormone signaling, and feedback loops involving leptin, myostatin, and incretins. Population simulations aligned closely with clinical trial responses, demonstrating how systems-level understanding can reconcile seemingly disparate endpoints.
This drive toward mechanistic fidelity is closely intertwined with the growing role of artificial intelligence and machine learning. Rather than replacing traditional pharmacometric approaches, AI is augmenting them in powerful ways. Presentations showcased variational autoencoders combined with neural ordinary differential equations for population modeling, offering scalable alternatives to classical nonlinear mixed-effects frameworks while preserving uncertainty quantification and handling complex latent variability. Machine-learning-enhanced structural model search tools (such as mlxModelFinder) accelerated discovery of appropriate compartmental or mechanistic structures.
Probabilistic PBPK frameworks for herb-drug interactions; exemplified by work on Banhasasim-tang with conventional GERD therapies used Monte Carlo simulations and marker-compound approaches to quantify content variability, parameter uncertainty, and clinical relevance. Even multidimensional representation scoring of real-world datasets (e.g., NHANES) illustrated how modern statistical and ML techniques can uncover hidden covariate structures that traditional methods might miss. The community is clearly embracing hybrid paradigms: mechanistic cores enriched by data-driven components, enabling both biological interpretability and predictive power.
Equally important at PAGE 2026 was the foregrounding of safety, toxicology, and ethical considerations. Late-stage attrition in drug development remains dominated by safety concerns, and the meeting reflected a growing recognition that efficacy modeling alone is insufficient. The European Commission’s roadmap toward phasing out animal testing for chemical safety assessments was referenced in context, emphasizing the ethical imperative to protect sentient beings while advancing industrial competitiveness through non-animal methods. This aligns with broader translational initiatives such as the FAIR project, which bridges healthy-volunteer safety and immunoactivation data to patient efficacy outcomes in respiratory infections. Multi-source databases integrating in vivo models, bronchoalveolar lavage, colony-forming units, and cytokine measurements support quantitative understanding of combination therapies (e.g., amoxicillin with novel agents like FLAMOD against *Streptococcus pneumoniae*). These efforts integrate host-drug-disease interplay—bacterial growth kinetics, immune modulation (CCL20), and compartmental PK—into unified frameworks.
Special populations received dedicated attention. Sophisticated pregnancy models were complemented by pharmacokinetic decision trees guiding the evaluation of infant systemic exposure through human milk. These trees systematically triage approaches—case reports, popPK, or PBPK—based on medication prevalence, safety profiles in adults and infants, and expected exposure levels, providing a practical roadmap for regulators, clinicians, and researchers. Reproductive medicine modeling stood out for its depth: multi-compartment follicle growth simulations (theca and granulosa cells, steroidogenesis pathways involving thousands of reactions and species) enabled individualized dosing algorithms for follitropin delta (recombinant FSH). Covariate effects of anti-Müllerian hormone (AMH) on maximal response were explicitly incorporated, with stochastic recruitment and dynamic sensitivity changes across a pool of follicles. Such models move beyond empirical dose-finding to mechanistic, patient-specific predictions of oocyte retrieval.
Clinical decision support emerged as a natural extension of these advances. The OptiThyDose platform exemplified this trend. Built on disease-specific pharmacometric models for congenital hypothyroidism and pediatric Graves’ disease, it generates individualized levothyroxine dosing recommendations by predicting FT4 trajectories, accounting for inter-individual variability, and visualizing target versus standard-dosing outcomes. Integration into routine workflows—initial assessment, blood sampling, model application, result review, and follow-up—addresses real-world scalability challenges: clinical and laboratory heterogeneity, medication complexity, and variability in care patterns. Similar principles underpinned herb-drug interaction platforms and lactation safety tools, demonstrating how model-informed approaches can translate into actionable clinical intelligence. This is by far the most ambitious and also the most translatable application I have witnessed in Modelling.
Throughout the meeting, posters on exposure metrics (AUC versus Cmax in continuous exposure-response relationships), global sensitivity analysis, and stochastic simulation reinforced the importance of robust methodological foundations. Discussions on hidden scalability challenges in patient journeys—practice patterns, disease severity, formulation differences, dosing habits, and visit schedules—reminded attendees that even the most elegant models must ultimately serve heterogeneous real-world settings.
Synthesizing these threads, PAGE 2026 painted a portrait of a discipline coming of age. The move from data description to mechanistic explanation is enabled by cumulative scientific progress; AI provides new tools for handling complexity without sacrificing interpretability; safety and ethical considerations are no longer peripheral but central design principles; and translational ambition is driving tools that directly support clinical decision-making in special populations and complex diseases.
As a first-time attendee, I left Dubrovnik with the idea on how good the PAGE organizing community organizes the parties. The field is not merely advancing technically; it is maturing philosophically—embracing complexity while remaining grounded in biological reality, prioritizing patient benefit, and confronting ethical responsibilities. The conversations, posters, and presentations I witnessed will shape my own thinking for years to come.
What I encountered surpassed them: a community not only deeply engaged in rigorous quantitative science but also actively steering pharmacometrics toward greater mechanistic depth, computationally aware and really strong on communal belongingness.
The stunning Adriatic backdrop provided a fitting stage for discussions that revealed a field in clear transition: from describing clinical data with relatively simple compartmental models to building explanatory, physiologically grounded frameworks that integrate decades of accumulated biological knowledge.
There is a silent shift in pharmacometrics from empirical description to mechanistic explanation, not toward pure machine learning or hybrid ODEs. This directly challenges the investment thesis that insilico AI will render deterministic PK/PD obsolete.
Mechanistic modeling dominated the scientific program. Pregnancy PBPK-PD frameworks for monoclonal antibodies integrated FcRn-mediated IgG recycling, placental transfer dynamics, and gestational physiology across trimesters, incorporating allometric scaling and in vitro binding data.
QSP platforms for metabolic disease linked multi-organ systems: CNS regulation, hepatic GLUT/insulin signaling, adipose energy balance, and gut hormone feedback: through differential equations.
There were parallel open source efforts that reconstructed advanced dissolution-absorption-metabolism (ADAM) models in open platforms like R, with explicit segmentation of the gastrointestinal tract, mechanistic handling of dissolution, precipitation, efflux, and metabolism. These were benchmarked against established tools such as Simcyp and PK-Sim, highlighting how structural assumptions influence predicted kinetics and underscoring the value of transparent, customizable implementations. And all things arise in the gut. Coming to open source there is a Rust based implementation for PKPD modelling and the cool part is that they have lots of different kinds of estimation and sampling method.
This evolution is not merely technological; it reflects the natural maturation of a discipline. In earlier eras, when clinical datasets were sparse and biomarkers limited, empirical or semi-mechanistic PK/PD models served as essential tools for characterizing exposure-response relationships. Today, with richer physiological understanding, multi-omics insights, and advanced computational power, researchers are constructing models that explain why phenomena occur.
The posters and presentations at PAGE 2026 made this shift extremely visible. Multiple groups presented sophisticated PBPK-PD models for pregnancy, capturing FcRn-mediated IgG recycling, placental transfer dynamics, and maternal-fetal concentration gradients for monoclonal antibodies such as Rozanolixizumab and Nipocalimab. These models integrated in vitro binding data, allometric scaling from cynomolgus monkey studies, and physiological changes across gestation weeks 14–35, with validation against both healthy volunteer and patient data, including compassionate-use cases. The result is not just better prediction but genuine mechanistic insight into how drug disposition changes in one of the most vulnerable populations.
The same spirit of mechanistic ambition appeared in Quantitative Systems Pharmacology (QSP) models of metabolism. Detailed multi-organ frameworks incorporated CNS neuron regulation, adipose energy balance, liver GLUT/insulin dynamics, muscle protein turnover, gut hormone signaling, and feedback loops involving leptin, myostatin, and incretins. Population simulations aligned closely with clinical trial responses, demonstrating how systems-level understanding can reconcile seemingly disparate endpoints.
This drive toward mechanistic fidelity is closely intertwined with the growing role of artificial intelligence and machine learning. Rather than replacing traditional pharmacometric approaches, AI is augmenting them in powerful ways. Presentations showcased variational autoencoders combined with neural ordinary differential equations for population modeling, offering scalable alternatives to classical nonlinear mixed-effects frameworks while preserving uncertainty quantification and handling complex latent variability. Machine-learning-enhanced structural model search tools (such as mlxModelFinder) accelerated discovery of appropriate compartmental or mechanistic structures.
Probabilistic PBPK frameworks for herb-drug interactions; exemplified by work on Banhasasim-tang with conventional GERD therapies used Monte Carlo simulations and marker-compound approaches to quantify content variability, parameter uncertainty, and clinical relevance. Even multidimensional representation scoring of real-world datasets (e.g., NHANES) illustrated how modern statistical and ML techniques can uncover hidden covariate structures that traditional methods might miss. The community is clearly embracing hybrid paradigms: mechanistic cores enriched by data-driven components, enabling both biological interpretability and predictive power.
Equally important at PAGE 2026 was the foregrounding of safety, toxicology, and ethical considerations. Late-stage attrition in drug development remains dominated by safety concerns, and the meeting reflected a growing recognition that efficacy modeling alone is insufficient. The European Commission’s roadmap toward phasing out animal testing for chemical safety assessments was referenced in context, emphasizing the ethical imperative to protect sentient beings while advancing industrial competitiveness through non-animal methods. This aligns with broader translational initiatives such as the FAIR project, which bridges healthy-volunteer safety and immunoactivation data to patient efficacy outcomes in respiratory infections. Multi-source databases integrating in vivo models, bronchoalveolar lavage, colony-forming units, and cytokine measurements support quantitative understanding of combination therapies (e.g., amoxicillin with novel agents like FLAMOD against *Streptococcus pneumoniae*). These efforts integrate host-drug-disease interplay—bacterial growth kinetics, immune modulation (CCL20), and compartmental PK—into unified frameworks.
Special populations received dedicated attention. Sophisticated pregnancy models were complemented by pharmacokinetic decision trees guiding the evaluation of infant systemic exposure through human milk. These trees systematically triage approaches—case reports, popPK, or PBPK—based on medication prevalence, safety profiles in adults and infants, and expected exposure levels, providing a practical roadmap for regulators, clinicians, and researchers. Reproductive medicine modeling stood out for its depth: multi-compartment follicle growth simulations (theca and granulosa cells, steroidogenesis pathways involving thousands of reactions and species) enabled individualized dosing algorithms for follitropin delta (recombinant FSH). Covariate effects of anti-Müllerian hormone (AMH) on maximal response were explicitly incorporated, with stochastic recruitment and dynamic sensitivity changes across a pool of follicles. Such models move beyond empirical dose-finding to mechanistic, patient-specific predictions of oocyte retrieval.
Clinical decision support emerged as a natural extension of these advances. The OptiThyDose platform exemplified this trend. Built on disease-specific pharmacometric models for congenital hypothyroidism and pediatric Graves’ disease, it generates individualized levothyroxine dosing recommendations by predicting FT4 trajectories, accounting for inter-individual variability, and visualizing target versus standard-dosing outcomes. Integration into routine workflows—initial assessment, blood sampling, model application, result review, and follow-up—addresses real-world scalability challenges: clinical and laboratory heterogeneity, medication complexity, and variability in care patterns. Similar principles underpinned herb-drug interaction platforms and lactation safety tools, demonstrating how model-informed approaches can translate into actionable clinical intelligence. This is by far the most ambitious and also the most translatable application I have witnessed in Modelling.
Throughout the meeting, posters on exposure metrics (AUC versus Cmax in continuous exposure-response relationships), global sensitivity analysis, and stochastic simulation reinforced the importance of robust methodological foundations. Discussions on hidden scalability challenges in patient journeys—practice patterns, disease severity, formulation differences, dosing habits, and visit schedules—reminded attendees that even the most elegant models must ultimately serve heterogeneous real-world settings.
Synthesizing these threads, PAGE 2026 painted a portrait of a discipline coming of age. The move from data description to mechanistic explanation is enabled by cumulative scientific progress; AI provides new tools for handling complexity without sacrificing interpretability; safety and ethical considerations are no longer peripheral but central design principles; and translational ambition is driving tools that directly support clinical decision-making in special populations and complex diseases.
As a first-time attendee, I left Dubrovnik with the idea on how good the PAGE organizing community organizes the parties. The field is not merely advancing technically; it is maturing philosophically—embracing complexity while remaining grounded in biological reality, prioritizing patient benefit, and confronting ethical responsibilities. The conversations, posters, and presentations I witnessed will shape my own thinking for years to come.
Pharmacometrics at PAGE 2026 was no longer just about fitting curves; it was about understanding systems, reducing uncertainty, protecting vulnerable populations, and translating knowledge into better outcomes. That is a trajectory worth following closely.
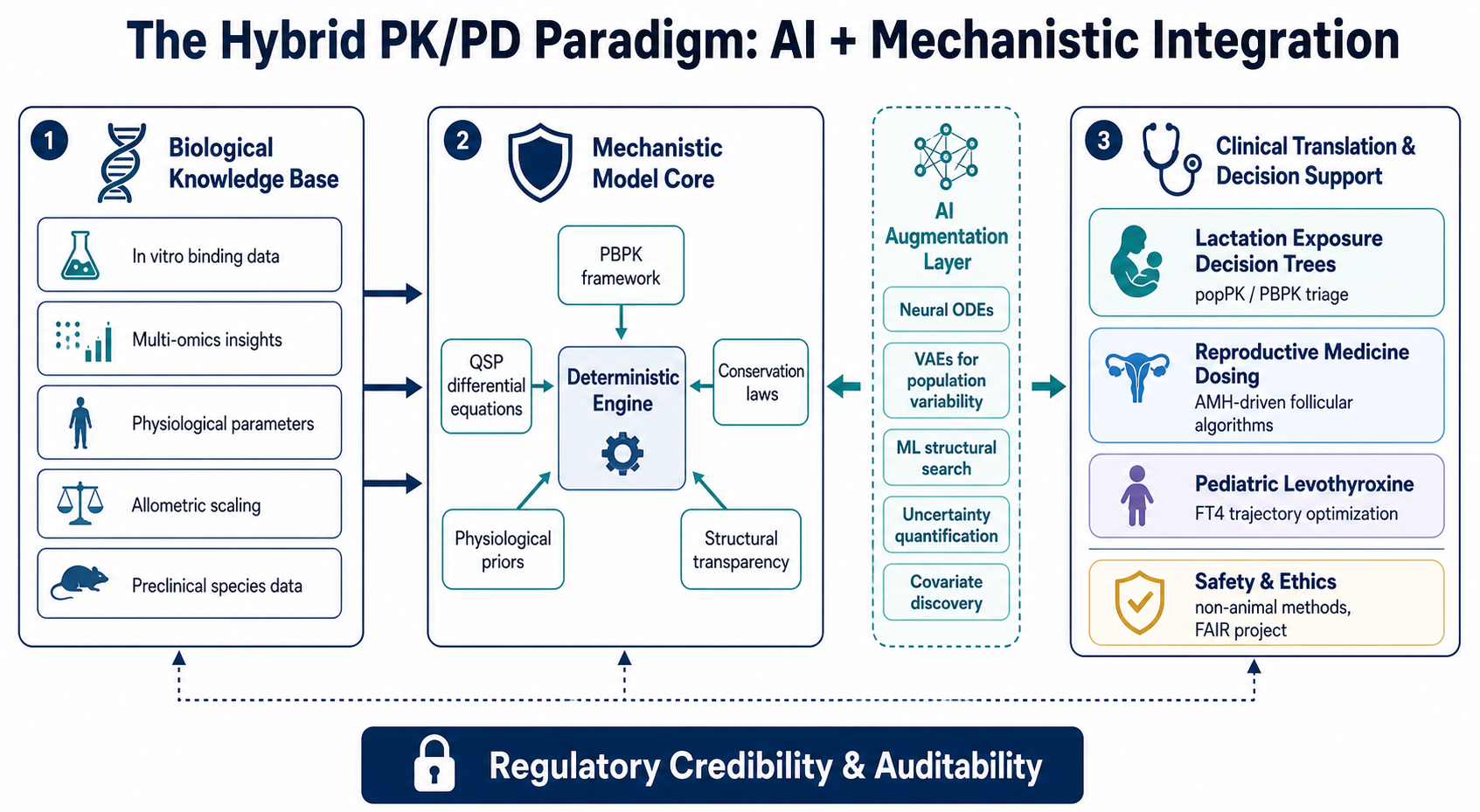

A great AI generated image by my colleagues!!.